Alcidion
Redesigning clinical task management for hospital nurses, where the consequence of a poor experience is not frustration but a patient waiting for care.
Position
Product designer
Scope
Research · UX design · Design system
Engagement type
Embedded research and design. No engineering sprint, no launch.
Output
Validated product direction, user research synthesis, and a design system foundation.
Domain
Clinical task management for hospital nurses across regulated Australian healthcare environments.
My role
Solo designer, embedded in the product team
I was brought in as the senior product designer to lead all research and design work on Smartpage. There was no existing design practice to lean on. I built the research approach from scratch, ran sessions directly with nurses in hospital settings, and translated what I found into a clear design direction for the product team to act on.
The problem
A system that worked against the people using it
Ward managers reported 5 to 7 missed urgent tasks per shift, classified as urgent, with direct risk of delayed patient care. Smartpage was built to replace paper-based pagers, but after years of feature additions it had become harder to use than the system it replaced.
Nurses were managing tasks across multiple views, mentally tracking urgency without the interface surfacing it, and working around the tool rather than through it. In a hospital ward, that friction does not just slow people down. It creates gaps.
Research
Two things nurses said, again and again
Research was done is 2 steps that I have brokendown below
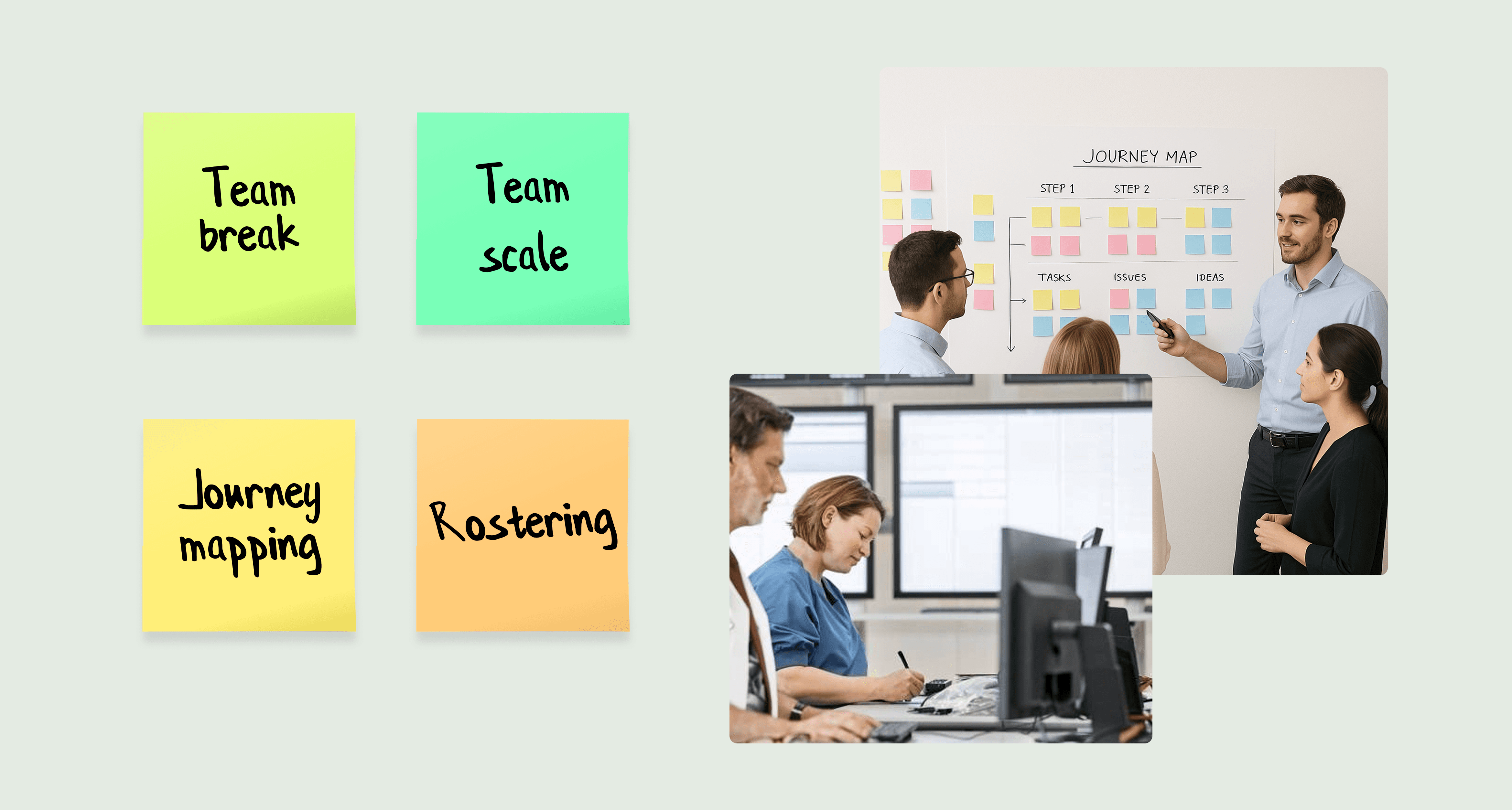
Step #1 Dogfooding - Mapping out the current onboarding.
Before speaking to nurses directly, I ran a dogfooding exercise with Alcidion's business consultants, the people who work inside hospital environments daily. They walked through Smartpage as if they were the end users, mapping the current experience against what ward teams actually need to do on a shift. This gave us a structured view of the task management workflow before we went into the field, and helped frame the right questions for the clinical interviews.
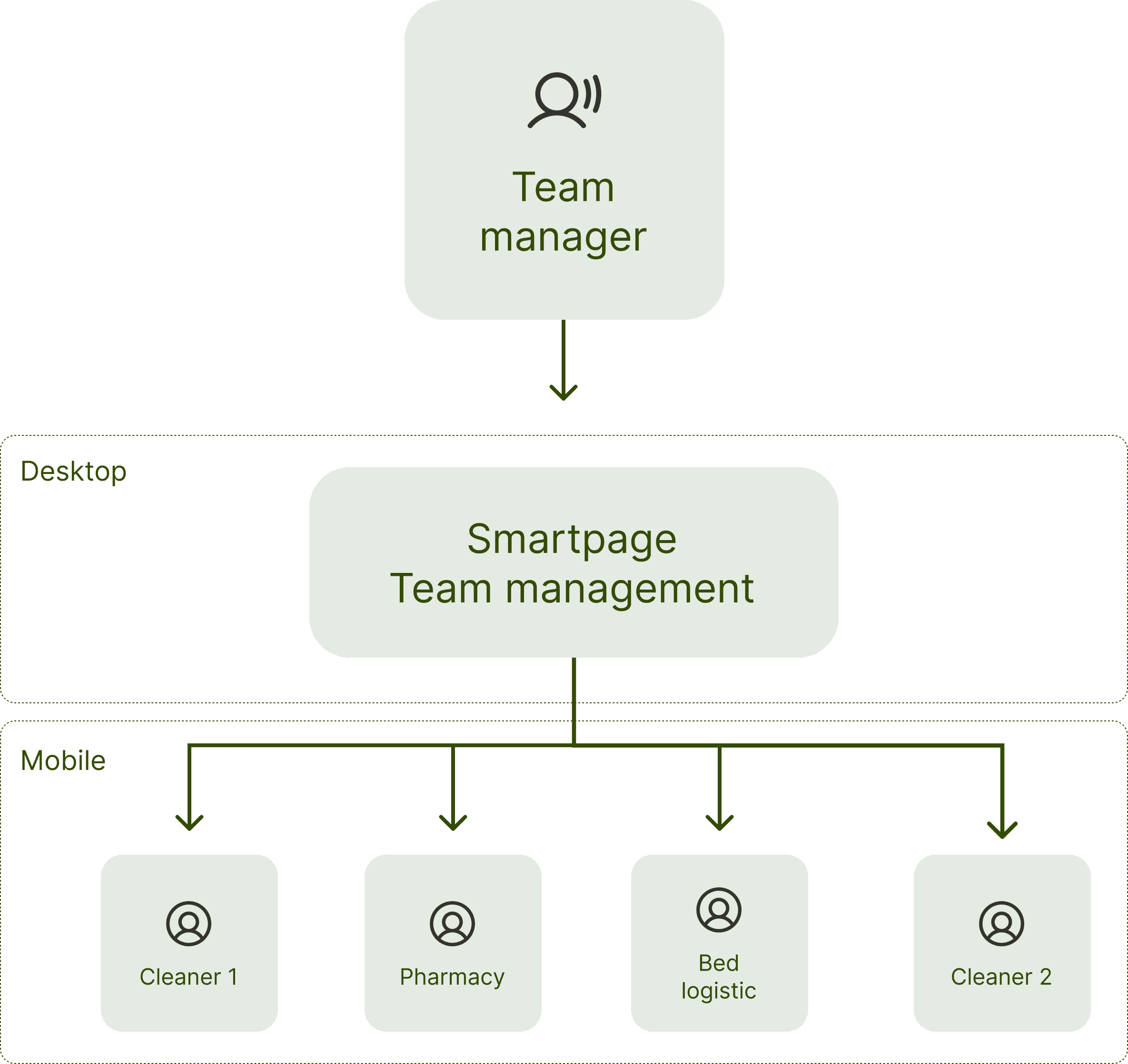
The core workflow we mapped: creating and assigning tasks, managing reassignments and cancellations, monitoring external requests, tracking team breaks for compliance, and maintaining visibility of staff locations and responsibilities across a shift.
Jobs to Be Done (Team Manager)
Create tasks.
Manage tasks: assign, reassign, cancel, and complete.
Manage workload: breaks, staffing balance.
Monitor and respond to external requests.
Define and maintain team structure: locations, roles, responsibilities.
Step #2 Contextual nurses interview
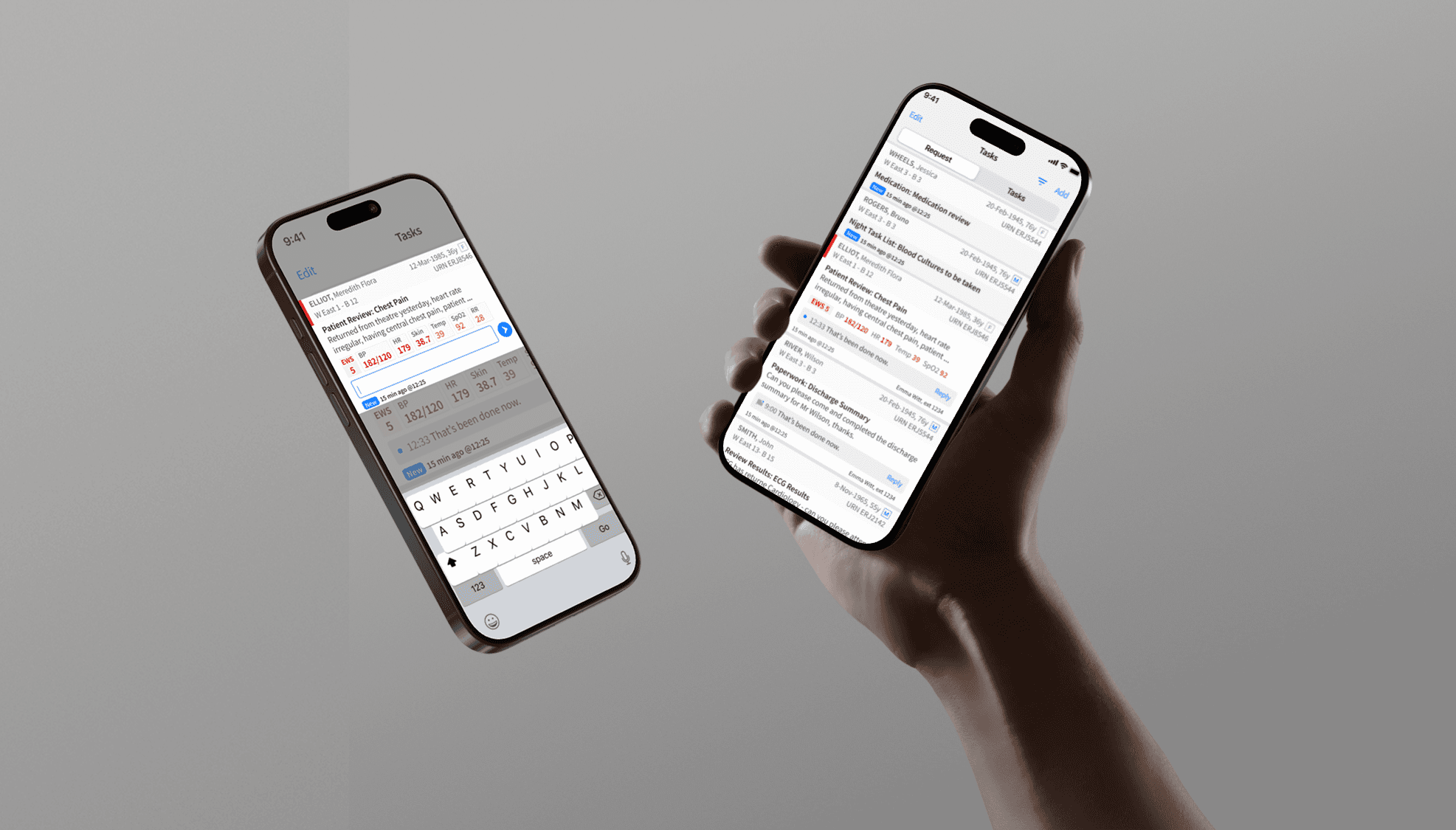
Four nurses participated in contextual sessions conducted mid-shift, in hospital settings, not in a meeting room. Clinical staff are genuinely difficult to access. Rigid shift patterns and patient care responsibilities mean research time is limited and must be earned. The sessions were focused and observational, watching nurses use Smartpage under real conditions rather than asking them to recall experiences retrospectively.
Two patterns came through consistently:
"I have no idea what is actually urgent right now. It all looks the same."
Registered Nurse, Wagga Wagga hospital
"Half the time I close the page by mistake and then I have no idea where I was."
Registered Nurse, Wagga Wagga hospital
The key insight
The tool had been designed around the message, not the person receiving it. Urgency was communicated through colour alone, with no haptic or audio signals to reinforce priority. In a fast-moving ward, colour is not enough. Staff needed to understand at a glance whether they were looking at a floor to clean or a respirator to move.
Design decisions
Three problems. Three clear responses.
01
Nurses could not tell what was urgent without reading every item
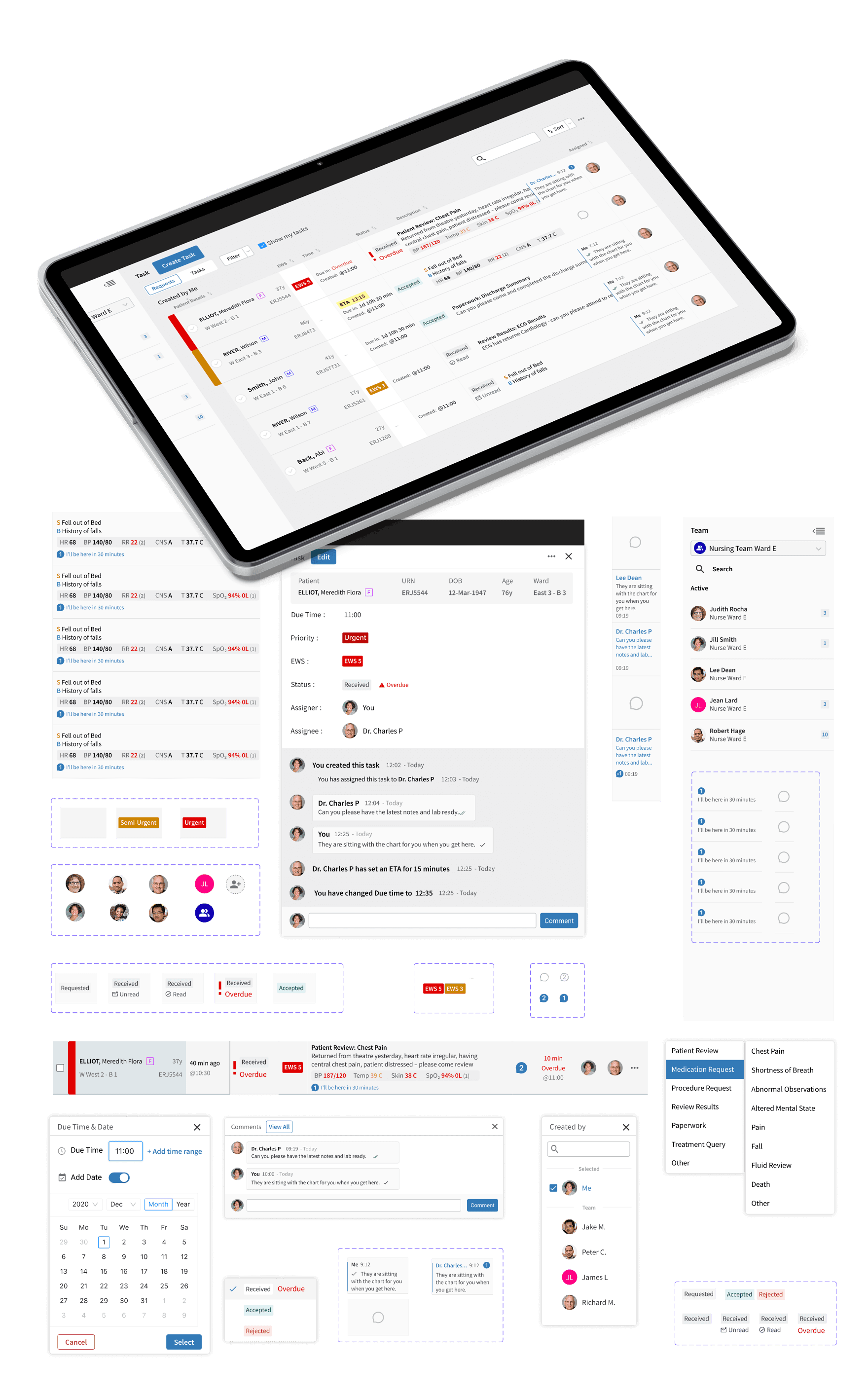
The task list showed everything at the same visual weight. I redesigned the priority hierarchy from the ground up, introducing a tiered visual system that surfaced urgency at the list level. Nurses could scan, not read, to triage what needed attention first.
02
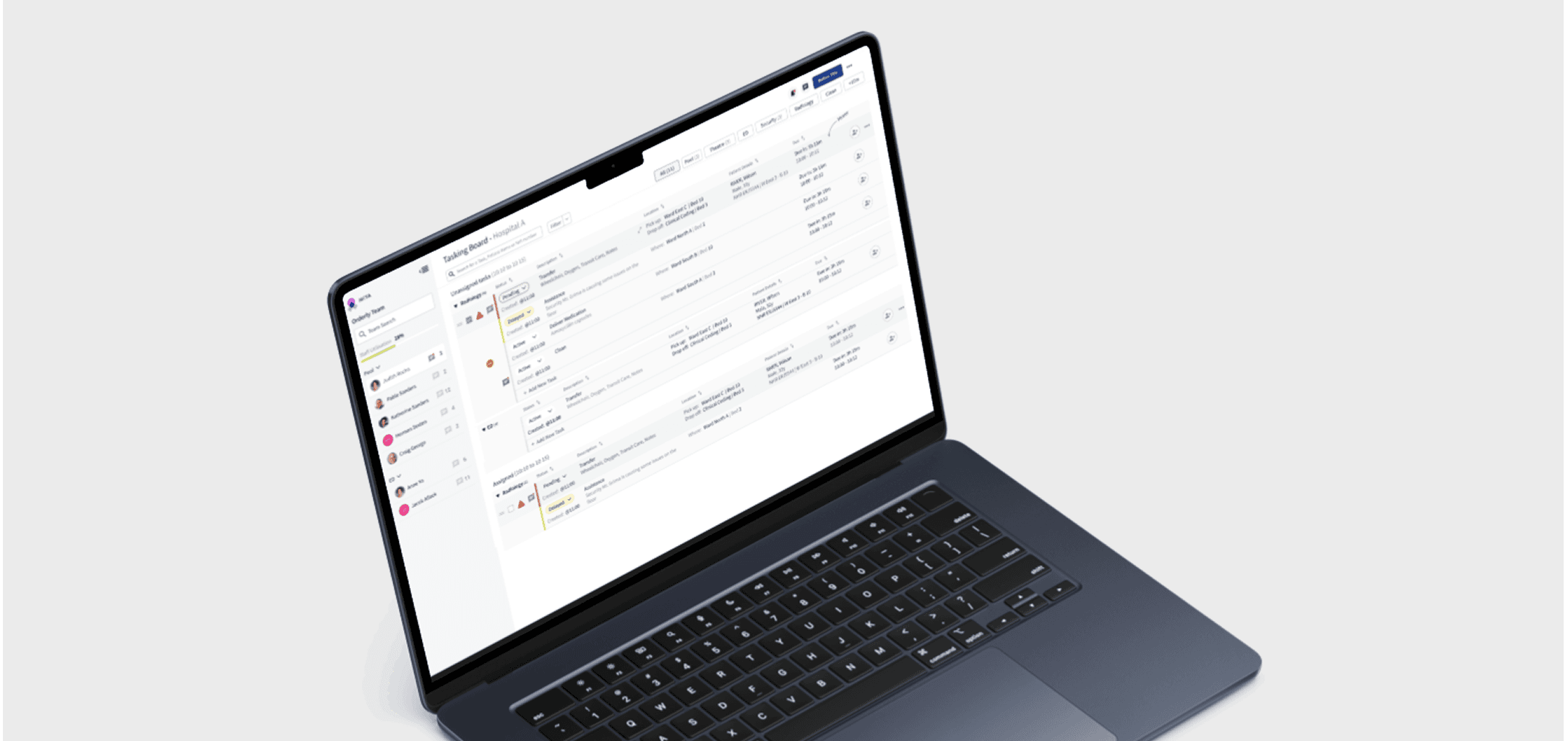
The ward view was invisible — nurses compensated with whiteboards
The product had no concept of the ward as a unit of work. Nurses needed to understand who was covering what across a full shift, not just their own queue. I introduced a ward-level view that gave charge nurses situational awareness without requiring them to chase individuals for updates.
03
Error recovery was too slow for a clinical environment
Accidental dismissals and navigation errors were common. In a fast-paced ward, having to re-navigate to find a task added real cognitive load at the worst possible moment. I redesigned the interaction model to make destructive actions harder to trigger accidentally and faster to recover from when they occurred.

The system underneath
Building a foundation the team could continue without me
Alongside the product work, I built a component library and design language for Smartpage. Alcidion had no shared design foundation across their products. This was the start of one.
What I built
A component library covering clinical task states, alert types, ward views, and navigation patterns — documented and ready to hand off.
Why it mattered
The team needed to keep building after I left. A design system meant future decisions would have a reference point, not a blank page.

What I'd do differently
Two things I would change
01
Push for post-launch measurement from day one
The engagement ended before the product shipped. I would now make success metrics part of the design brief at the start, not a conversation for after launch. Without them, you have no way to know if the direction you validated was the right call.
02
Bring clinical governance stakeholders into the process earlier
I got access to nurses early, but governance stakeholders came in much later. Their constraints shaped decisions that would have been better surfaced in the research phase. Regulated environments need those conversations at the start, not the end.